Coronary Artery Disease Diagnosis Treatment: Understanding Pathophysiology, Risk Factors. Drugs for the Treatment of Coronary Artery Disease: Mechanisms of action of drugs used for CAD, Contraindications, and Drug Interactions.
Introduction
Coronary artery disease (CAD), also known as coronary heart disease or atherosclerosis, is a leading cause of death worldwide. It occurs when plaque builds up in the coronary arteries, restricting blood flow to the heart muscle. Understanding the pathophysiology, risk factors, diagnosis, and treatment of CAD is crucial for effective prevention and management. In this article, we will delve into the intricate details of CAD, its various aspects, and how to reduce its risk and manage its symptoms.
CAD is a significant cardiovascular condition that requires a comprehensive treatment approach to manage symptoms, reduce complications, and improve overall heart health. Several medications play a crucial role in the management of CAD, each targeting different aspects of the disease process. In this article, we will explore the drugs commonly used for CAD treatment, their modes of action, contraindications, and potential drug interactions.

Pathophysiology of Coronary Artery Disease.
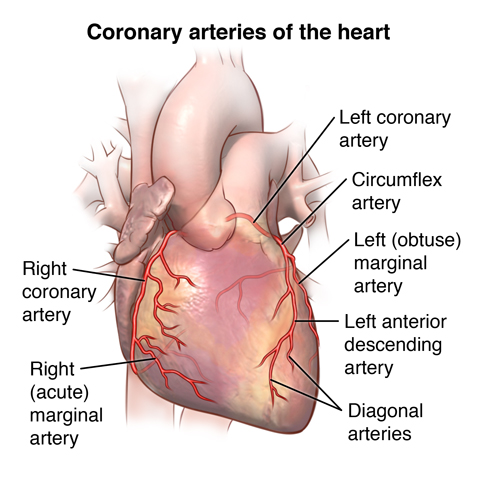
The pathophysiology of coronary artery disease begins with the accumulation of fatty deposits, cholesterol, and calcium on the inner walls of the coronary arteries. Over time, these deposits form atherosclerotic plaques, leading to a condition called atherosclerosis. The plaques narrow and harden the arteries, restricting blood flow to the heart muscle, which can result in various clinical manifestations, including stable angina or acute coronary syndrome (ACS).
Risk Factors for Coronary Artery Disease.
Several risk factors contribute to the development of CAD, including modifiable and non-modifiable factors. Modifiable risk factors include hypertension, dyslipidemia (high blood fats), smoking, diabetes mellitus, obesity, physical inactivity, and an unhealthy diet high in saturated fats and cholesterol. Non-modifiable risk factors include age, gender (men are at higher risk than premenopausal women), and family history of CAD.
Job Stress and its Link to CAD.
Recent research suggests that chronic job stress may also play a role in increasing the risk of developing CAD. Prolonged stress can lead to unhealthy coping mechanisms such as smoking, excessive alcohol consumption, and poor dietary choices. Additionally, stress activates the sympathetic nervous system, leading to increased heart rate and blood pressure, which can further contribute to the progression of atherosclerosis.
Ways to Reduce CAD Risk.
To reduce the risk of CAD, individuals can adopt a heart-healthy lifestyle. Regular physical activity, a balanced diet rich in fruits, vegetables, whole grains, and lean proteins, maintaining a healthy weight, managing stress through relaxation techniques, and quitting smoking can significantly lower the risk of CAD.
Signs and Symptoms of Coronary Artery Disease.
The signs and symptoms of CAD can vary depending on the severity and location of the blockages in the coronary arteries. Common symptoms include chest pain or discomfort (angina), shortness of breath, fatigue, palpitations, and dizziness. However, it’s important to note that some individuals, especially women, may experience atypical symptoms such as nausea, back or jaw pain, and profound fatigue.
Symptoms of CAD in Women.
Women may experience different symptoms compared to men, and their symptoms are often misattributed to other conditions. Women with CAD may present with atypical symptoms, as mentioned earlier, which can delay diagnosis and appropriate management. Healthcare providers need to be aware of these gender-specific differences to ensure timely and accurate diagnosis and treatment.
Blood Fats and Coronary Artery Disease.
Elevated blood fat levels, specifically LDL cholesterol and triglycerides, contribute to the development of atherosclerotic plaques in the coronary arteries. Lowering LDL cholesterol through lifestyle modifications and medications, such as statins, has been shown to reduce the risk of CAD and its complications.
Genetics of Coronary Artery Disease.
Genetics also play a role in the development of CAD. Individuals with a family history of CAD are at increased risk. Certain genetic variants have been associated with a higher risk of CAD, but genetic testing for CAD is not yet routine clinical practice. Nevertheless, knowing about family history can help in risk assessment and making informed lifestyle choices.
Diagnosis of Coronary Artery Disease.
The diagnosis of CAD involves a combination of patient history, physical examination, and various diagnostic tests. Non-invasive tests, such as electrocardiogram (ECG or EKG), stress tests, and echocardiograms, can provide valuable information about the heart’s function and blood flow. Invasive tests, such as coronary angiography, involve the injection of contrast dye into the coronary arteries to visualize any blockages.
Stable Angina and Acute Coronary Syndrome.
Stable angina is a common symptom of CAD and is characterized by predictable chest pain or discomfort that occurs with physical exertion and subsides with rest or medication. In contrast, acute coronary syndrome (ACS) refers to a sudden and potentially life-threatening reduction in blood flow to the heart due to a ruptured plaque or blood clot formation. ACS includes unstable angina, non-ST-segment elevation myocardial infarction (NSTEMI), and ST-segment elevation myocardial infarction (STEMI).
Diagnosis of Acute Coronary Syndrome.
Prompt diagnosis of ACS is critical for initiating appropriate treatment. Medical professionals use a combination of patient history, ECG, cardiac biomarkers (such as troponin), and imaging tests, such as coronary angiography, to diagnose and classify ACS.
Risk Assessment: Framingham Score and Polygenic Score.
Risk assessment tools like the Framingham Risk Score estimate the 10-year risk of developing CAD based on various risk factors, including age, cholesterol levels, blood pressure, and smoking status. Additionally, emerging research on polygenic scores involves analyzing multiple genetic markers to determine an individual’s genetic risk for CAD.
Prevention of Coronary Artery Disease.
Preventing CAD involves lifestyle modifications, as mentioned earlier, along with regular medical check-ups, managing underlying medical conditions like hypertension and diabetes, and adhering to prescribed medications, especially if high cholesterol levels persist despite lifestyle changes.
Medication Treatment for Coronary Artery Disease.
Medications used in the treatment of CAD include antiplatelet agents (such as aspirin), beta-blockers, ACE inhibitors or ARBs, statins, and nitroglycerin. These medications help manage symptoms, prevent blood clots, lower blood pressure, and reduce cholesterol levels, ultimately improving overall heart health.
Drugs for the Treatment of Coronary Artery Disease: Mechanisms, Contraindications, and Drug Interactions
Antiplatelet Agents:
Examples: Aspirin, Clopidogrel, Ticagrelor
Mode of Action: Antiplatelet agents inhibit the activation and aggregation of platelets, preventing the formation of blood clots within coronary arteries.
Contraindications: Allergy to the drug, active bleeding, bleeding disorders, recent major surgery, history of gastrointestinal ulcers.
Drug Interactions: Aspirin may interact with anticoagulants like warfarin, increasing the risk of bleeding. Clopidogrel and Ticagrelor may interact with certain proton pump inhibitors (PPIs) used for acid reflux, potentially reducing their effectiveness.
Beta-Blockers:
Examples: Metoprolol, Atenolol, Carvedilol
Mode of Action: Beta-blockers block the action of adrenaline on the heart, reducing heart rate and blood pressure, thereby decreasing the workload on the heart.
Contraindications: Severe heart failure, heart block, asthma, severe chronic obstructive pulmonary disease (COPD).
Drug Interactions: Beta-blockers may interact with other medications that lower blood pressure, such as calcium channel blockers, leading to an excessive drop in blood pressure.
ACE Inhibitors (Angiotensin-Converting Enzyme Inhibitors):
Examples: Lisinopril, Enalapril, Ramipril
Mode of Action: ACE inhibitors dilate blood vessels, reducing blood pressure and decreasing the workload on the heart. They also help protect the heart from the harmful effects of angiotensin II.
Contraindications: Allergy to ACE inhibitors, history of angioedema, bilateral renal artery stenosis.
Drug Interactions: ACE inhibitors may interact with nonsteroidal anti-inflammatory drugs (NSAIDs), leading to reduced blood pressure-lowering effects and potential kidney problems.
ARBs (Angiotensin Receptor Blockers):
Examples: Losartan, Valsartan, Irbesartan
Mode of Action: ARBs block the action of angiotensin II, a hormone that causes blood vessels to constrict, leading to vasodilation and lowered blood pressure.
Contraindications: Allergy to ARBs, history of angioedema, bilateral renal artery stenosis.
Drug Interactions: ARBs may interact with potassium-sparing diuretics or potassium supplements, leading to increased potassium levels in the blood (hyperkalemia).
Statins:
Examples: Atorvastatin, Simvastatin, Rosuvastatin
Mode of Action: Statins inhibit an enzyme involved in cholesterol synthesis, reducing LDL (low-density lipoprotein) cholesterol levels in the blood.
Contraindications: Liver disease, pregnancy, breastfeeding.
Drug Interactions: Statins may interact with certain medications, such as fibrates or certain antibiotics, increasing the risk of muscle damage (rhabdomyolysis).
Nitroglycerin:
Examples: Sublingual nitroglycerin tablets, Nitroglycerin spray
Mode of Action: Nitroglycerin relaxes and widens blood vessels, increasing blood flow to the heart and relieving angina (chest pain).
Contraindications: Use of erectile dysfunction medications (like sildenafil) or other medications that lower blood pressure.
Drug Interactions: Nitroglycerin may interact with PDE5 inhibitors (used for erectile dysfunction), leading to a dangerous drop in blood pressure.
Conclusion:
Coronary artery disease is a complex condition with multiple contributing factors. By understanding its pathophysiology, risk factors, diagnosis, and treatment options, individuals can take proactive steps to reduce their risk and manage the disease effectively. Emphasizing lifestyle changes and regular medical check-ups, along with appropriate medication, can significantly improve outcomes and enhance overall heart health.
The drugs used in the treatment of coronary artery disease play essential roles in managing symptoms, preventing complications, and improving the overall quality of life for affected individuals. Understanding the mechanisms, contraindications, and potential drug interactions associated with these medications is crucial for healthcare providers to ensure safe and effective CAD management. Patients should always inform their healthcare providers about any existing medical conditions, medications, or supplements they are taking to avoid adverse interactions and ensure the best possible treatment outcomes.

Leave a Reply